Drug Interaction Type Identifier
Scenario Input
Describe the interaction scenario or select from common examples.
Analysis Result
Enter a scenario and click Analyze to see the classification.
Management Strategy:
Imagine you are taking two different medications. One makes the other work too strongly, causing side effects. The other makes it barely work at all. Why does this happen? It usually comes down to one of two things: how your body handles the drug, or how the drug affects your body.
This is the core difference between pharmacokinetic and pharmacodynamic drug interactions. Understanding this split isn’t just academic jargon; it is the key to staying safe when you take multiple prescriptions. In the UK alone, adverse drug events account for a significant portion of hospital admissions. Many of these are preventable if we know whether an interaction changes the amount of drug in your blood or the effect that drug has on your cells.
The Core Difference: Body vs. Drug
To keep this simple, think of it like a car trip. Pharmacokinetics (PK) is what your body does to the drug. It covers Absorption, Distribution, Metabolism, and Excretion-often called ADME. This determines how much medicine actually reaches your target tissue.
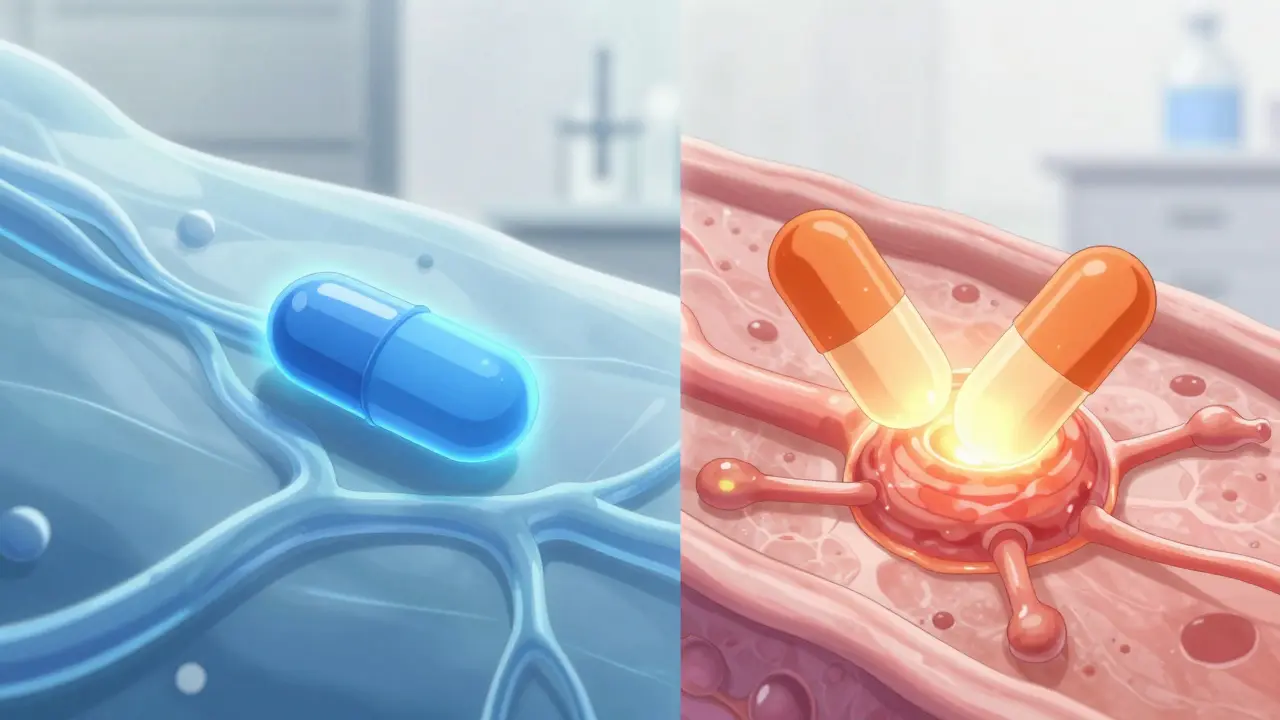
Pharmacodynamics (PD) is what the drug does to your body. This describes the biochemical effects, like binding to receptors to lower blood pressure or stop pain. If PK is about getting the driver to the destination, PD is about how they drive once they get there.
When two drugs interact, they either mess with the journey (PK) or crash into each other at the destination (PD). Knowing which type you are dealing with helps doctors decide whether to adjust the dose or avoid the combination entirely.
How Pharmacokinetic Interactions Work
Pharmacokinetic interactions change the concentration of a drug in your bloodstream. They don’t necessarily change how the drug works chemically, but they change how much of it is available to work. These interactions fall into four main buckets based on the ADME process.
- Absorption: Some drugs block others from entering the bloodstream. For example, antacids can reduce the absorption of quinolone antibiotics by up to 90%. If you take them together, the antibiotic might not fight the infection effectively.
- Distribution: Drugs travel in the blood attached to proteins. If Drug A kicks Drug B off its protein seat, more free Drug B circulates in the body. Warfarin displacement by phenylbutazone is a classic case, potentially increasing bleeding risk significantly.
- Metabolism: This is the most common source of PK interactions. Your liver uses enzymes to break down drugs. The Cytochrome P450 enzyme family, especially CYP3A4, handles about 75% of these metabolic interactions. If Drug A inhibits the enzyme that breaks down Drug B, levels of Drug B can skyrocket. Clarithromycin inhibiting CYP3A4 can increase simvastatin exposure tenfold, raising the risk of muscle damage.
- Excretion: Kidneys remove drugs from the body. Probenecid, for instance, can reduce penicillin clearance by half, keeping the antibiotic in the system longer.
The good news about PK interactions is that they are often predictable. Because they rely on specific enzymes or transporters, we can often manage them by adjusting doses or monitoring blood levels.
How Pharmacodynamic Interactions Work
Pharmacodynamic interactions occur when two drugs affect the same physiological system or receptor site. Here, the amount of drug in your blood might be normal, but the combined effect on your body is problematic. There are three main types of PD interactions.
- Additive Effects: Two drugs do the same thing, so the result is 1 + 1 = 2. Taking warfarin (a blood thinner) and aspirin (which also affects clotting) increases bleeding risk because both attack the clotting mechanism from different angles.
- Synergistic Effects: The combined effect is greater than the sum of individual parts (1 + 1 = 3). Mixing sildenafil with nitrates can cause severe, life-threatening hypotension because they amplify each other’s vasodilating effects.
- Antagonistic Effects: One drug cancels out the other. Naloxone reverses opioid overdose by blocking opioid receptors. Similarly, beta-blockers can cancel out the heart-rate-increasing effects of beta-agonists used for asthma.
PD interactions are particularly common with central nervous system drugs. According to recent reviews, they account for 85% of CNS drug interactions, especially among antidepressants, antipsychotics, and opioids. Unlike PK interactions, you can’t always fix a PD interaction by lowering the dose. Sometimes, you simply cannot take the two drugs together.
Key Differences at a Glance
To help you distinguish between the two, here is a comparison of their primary characteristics.
| Feature | Pharmacokinetic (PK) | Pharmacodynamic (PD) |
|---|---|---|
| Definition | What the body does to the drug | What the drug does to the body |
| Mechanism | Alters drug concentration (ADME) | Alters drug response/receptor activity |
| Predictability | Often predictable via enzyme profiles | Can be complex and less predictable |
| Management | Dose adjustment, therapeutic monitoring | Avoid combination, monitor clinical signs |
| Common Examples | CYP450 inhibition/induction | Additive sedation, opposing BP effects |
Why Management Strategies Differ
The way clinicians handle these interactions depends heavily on which type they are. Dr. David E. Golan notes that PK interactions shift the dose-response curve horizontally (changing concentration), while PD interactions shift it vertically (changing maximal effect).
For pharmacokinetic interactions, the strategy is often modification. If you are taking a narrow therapeutic index drug like warfarin or digoxin, doctors will use Therapeutic Drug Monitoring (TDM) to check blood levels. They might reduce the dose of the interacting drug or space out the timing. For example, separating the intake of antacids and antibiotics by two hours can prevent absorption issues.
For pharmacodynamic interactions, avoidance is frequently the only safe option. You cannot easily "dose" your way out of serotonin syndrome caused by mixing MAO inhibitors and SSRIs. Similarly, combining certain cardiovascular agents can lead to dangerous drops in blood pressure that no amount of careful dosing can fully mitigate without risking treatment failure. The UK Specialist Pharmacy Service emphasizes that understanding the mechanism is crucial: PK interactions often need monitoring, while PD interactions often demand avoidance.

Real-World Scenarios and Risks
Let’s look at some concrete examples to see how this plays out in daily life.
The Statin and Antibiotic Combo: Simvastatin is metabolized by CYP3A4. If you start taking clarithromycin (a strong CYP3A4 inhibitor) for an infection, your simvastatin levels can rise dramatically. This is a PK interaction. The solution? Switch to a statin not metabolized by CYP3A4, or temporarily pause the statin, or drastically reduce the dose.
The Blood Pressure Puzzle: NSAIDs (like ibuprofen) can reduce the effectiveness of ACE inhibitors (like lisinopril) by interfering with prostaglandin pathways. This is a PD interaction. The blood pressure medication is still in your system at the right level, but the body’s response is blunted. The result? Uncontrolled hypertension. The fix isn’t just raising the ACE inhibitor dose; it might require switching to a different pain relief option.
The Sedative Slip: Combining benzodiazepines and opioids is a PD interaction involving additive CNS depression. Both drugs slow breathing. Even at standard doses, the combination can suppress respiratory drive enough to cause fatal overdose. This requires strict avoidance or extreme caution with continuous monitoring.
Emerging Tools for Safety
We are getting better at predicting these interactions. Electronic health records now flag thousands of high-severity interactions automatically. New guidelines from the FDA and EMA require testing for interactions with major CYP enzymes and transporters before drugs reach the market.
Pharmacogenomics is also changing the game. By testing your genes, doctors can predict how your CYP450 enzymes function. If you are a "poor metabolizer" for CYP2D6, you are at higher risk for PK interactions with drugs processed by that enzyme. Meanwhile, AI models are being trained to predict PD interactions with increasing accuracy, helping to identify dangerous combinations that haven’t been clinically proven yet.
Ultimately, whether an interaction is PK or PD, the goal is the same: maximizing benefit while minimizing harm. Always review your medication list with a pharmacist or doctor, especially when starting new treatments. They can spot these hidden clashes before they become health crises.
Can a drug interaction be both pharmacokinetic and pharmacodynamic?
Yes, it is possible for a single pair of drugs to have both types of interactions. For example, one drug might inhibit the metabolism of another (PK), increasing its concentration, while also acting on the same receptor pathway (PD), amplifying the effect. However, clinicians usually focus on the dominant mechanism to determine management strategy.
Which type of interaction is more dangerous?
Neither is inherently more dangerous; both can be life-threatening depending on the drugs involved. PK interactions can lead to toxic accumulation of drugs, while PD interactions can cause immediate physiological collapse (like respiratory depression). PD interactions are often harder to reverse quickly because they involve direct biological effects rather than just clearing a toxin from the blood.
How long do pharmacokinetic interactions last?
The duration depends on the half-life of the interacting drugs and the nature of the enzyme inhibition or induction. Enzyme induction (speeding up metabolism) can take weeks to develop and weeks to reverse after stopping the inducing drug. Enzyme inhibition (slowing down metabolism) often happens within days and resolves relatively quickly once the inhibitor is cleared from the body.
Do over-the-counter supplements cause drug interactions?
Absolutely. Supplements like St. John’s Wort can induce CYP3A4 enzymes, reducing the effectiveness of many prescription drugs (a PK interaction). Grapefruit juice inhibits CYP3A4, potentially increasing drug levels. Always treat supplements as potential interactors and disclose them to your healthcare provider.
How can I check for drug interactions myself?
You can use reputable online databases like the UK Specialist Pharmacy Service (SPS) or Medscape. However, these tools provide general information. Your personal genetics, kidney function, and other health conditions influence how you react. Always consult a pharmacist or doctor for personalized advice, especially before making any changes to your regimen.